
Pneumocystis Pneumonia and
Cavalier King Charles Spaniels

Cavalier King Charles spaniels are predisposed to develop pneumocystis pneumonia (also referred to as pneumocystis carinii pneumonia [PCP], and pneumocystosis) a form of pneumonia caused by a fungus, commonly found in the lungs of most all dogs but which can infect the lungs of dogs with weak immune systems. It can cause severe, life-threatening pneumonia in susceptible dogs, such as the cavalier, if not diagnosed and treated at an early stage.
Pneumocystis pneumonia was first reported about in a CKCS in a 1996 article, and several veterinary research articles have been written about it since then. In this November 2017 article analyzing 43 previous published cases, cavaliers represented nearly 40% of all dogs reported with PCP. Dachshunds also are known to be predisposed to pneumocystis pneumonia as a breed-specific immune system disorder, and Yorkshire terriers to a lesser extent.
A comprehensive case study report of this disorder in a young cavalier is this December 2023 Clinician's Brief article.
RETURN TO TOP
What It Is
Pneumocystis pneumonia is caused by a fungus, pneumocystis jirovecii, which is commonly found in the lungs of dogs but which can cause infection of the lungs of dogs which have immune system deficiencies.
Inherited immune system deficiency is suspected as a cause in the CKCS breed, in part, because in a 2009 Australian study, a pair of cavalier littermates were diagnosed with pneumocystis pneumonia. In the cavalier, this infection has been diagnosed in young and older dogs.
In a 2001 UK study of the DNA of pneunocystis cysts taken from a cavalier, the researchers reported detecting a unique form of pneumocystis, stating:
"We have therefore shown that this dog was infected with a genetically distinct form of Pneumocystis and propose that Pneumocystis infecting a canine host be referred to as Pneumocystis canis. It is also proposed that the two forms be temporarily designated Type A and Type B while awaiting further clarification of their relationship."
RETURN TO TOP
Symptoms
The most common early symptoms of pneumocystis pneumonia are a non-productive cough, very rapid breathing, shortness of breath, and possibly rapid heart rate. As the disorder progresses, the dog may develop inflammation in the mouth, including lesions, poor appetite, and exercise intolerance, but with a normal body temperature. Also, the dog's breathing becomes more and more labored.
In a March 2018 clinical report, symptoms in an infected CKCS included: persistent dyspnea, inappetence, and lethargy for two weeks, high respiratory rate (140 bpm), no heart murmur; x-rays showed a moderately diffuse interstitial lung pattern suggestive of interstitial pneumonia or possibly pulmonary edema; the right heart was prominent, and pulmonary artery enlargement was suspected. An echocardiogram revealed trivial to mild mitral valve regurgitation with no left-sided chamber enlargement, moderate enlargement of the right atrium and ventricle with moderate tricuspid valve regurgitation, and a moderately dilated pulmonary artery with severely increased pulmonary arterial pressure.
Note that mouth lesions also are symptomatic of eosinophilic stomatitis, another immune-related disorder to which the CKCS is predisposed. Also, chronic ulcerative paradental stomatitis (CUPS), to which cavaliers are "over-represented", includes mouth inflammation and ulcers as symptoms.
RETURN TO TOP
Diagnosis
In this March 2022 article, the authors summarized the basis for suspecting that PCP is the correct diagnosis:
"Factors including breed, age, evidence of impaired immunity, presence of chronic co-infections, as well as a history of long-standing therapy-resistant respiratory disorders are essential considerations for including pneumocystosis as a diagnostic possibility, or for making a presumptive clinical diagnosis."
 There
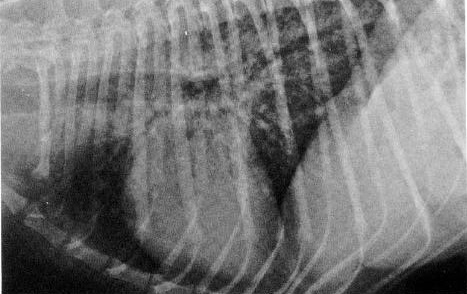
are several options available for diagnosis of PCP. An x-ray
should reveal a fine, net-like pattern of matter in the lungs, referred to as a
"generalized interstitial lung pattern" (see at left).
High resolution computed tomography (HRCT) will be more effective in providing
an accurate diagnosis than a plain radiograph. In a
March 2018 article, UK
clinicians reported that:
There
are several options available for diagnosis of PCP. An x-ray
should reveal a fine, net-like pattern of matter in the lungs, referred to as a
"generalized interstitial lung pattern" (see at left).
High resolution computed tomography (HRCT) will be more effective in providing
an accurate diagnosis than a plain radiograph. In a
March 2018 article, UK
clinicians reported that:
"Thoracic CT [computed tomography] revealed ground glass opacity of the pulmonary parenchyma with a diffuse or multifocal distribution. The severity of this pattern was variable. Less consistent imaging findings included parenchymal bands, bronchial dilation and signs consistent with pulmonary hypertension."
In the March 2022 article, the authors added that the x-ray's interstitial lung pattern and CT's ground glass opacities, are "often accompanied by right side heart enlargement (cor pulmonale) and echocardiographic evidence for pulmonary hypertension".
The examining veterinarian should perform a bronchoalveolar lavage (BAL) under anestheseia, a procedure in which a bronchoscope is passed through the mouth or nose into the lungs and fluid is squirted into a small part of the lung and then recollected for microscopic examination of the cellular make-up of the fluid. If successful, the exam should show the presence of pneumocystis jirovecii organisms.
Polymerase chain reaction (PCR) analysis, to confirm
the presence of pneumocystis infection, is a
 diagnostic technique used
which makes copies of a specific DNA region from a BAL sample. See this
March 2018 article.
diagnostic technique used
which makes copies of a specific DNA region from a BAL sample. See this
March 2018 article.
In a March 2025 article, a 16-month-old cavalier King Charles spaniel with a history of progressive rapid respiratory rate (tachypnea), increased respiratory effort, and weight loss that had failed to respond to antimicrobial and antifungal treatments. The dog was diagnosed with pneumocystis pneumonia by polymerase chain reaction performed from an oropharyngeal swab. The clinicians reported that this is the first case report documenting pneumocystis pneumonia diagnosed via oropharyngeal swab.
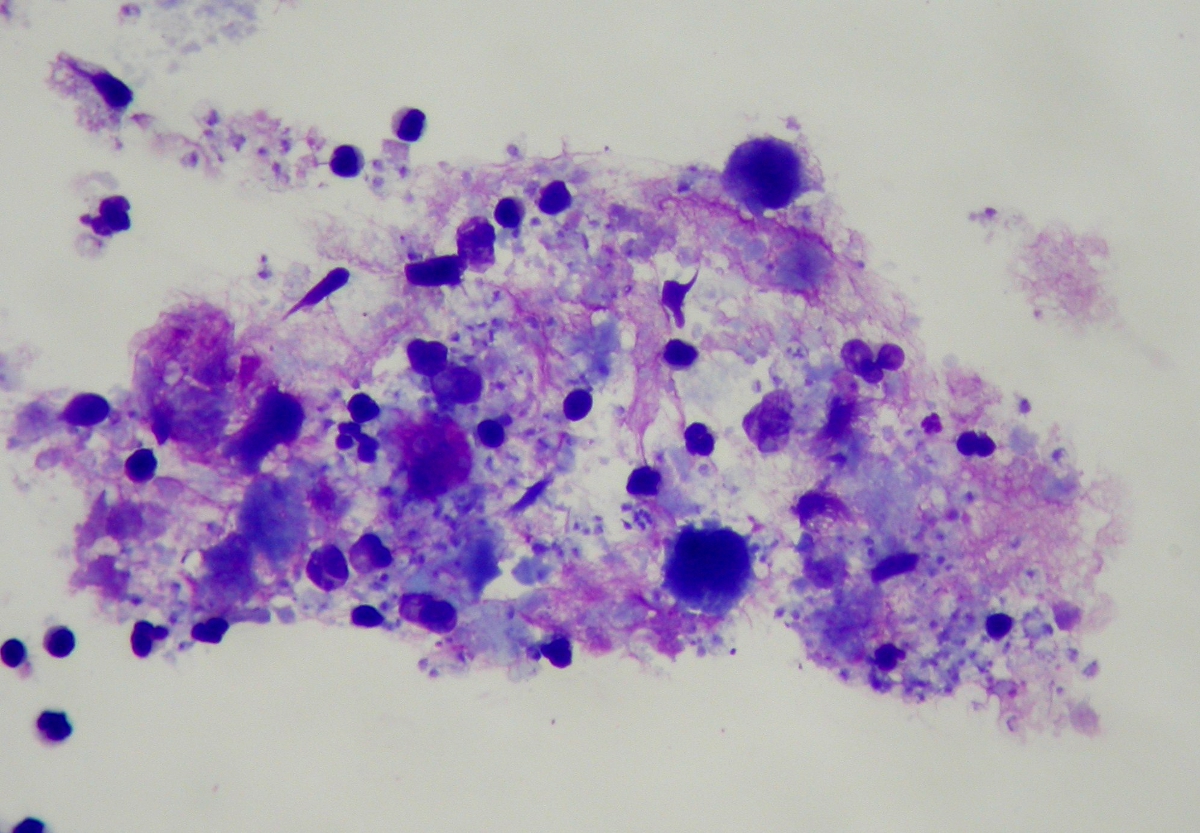
However, definitive diagnosis can be difficult, and BALs may be unhelpful. A more reliable alternative to the BAL is to perform a fine needle biopsy or aspirate, by inserting a needle into the lung to collect a sample of the affected lung tissue. But, this procedure may increase risk of complications, especially in dogs whose respiratory function is already severely compromised. Also, as with the BAL, this diagnostic procedure does not always detect the fungus. (The photo at the right shows pneumocystis jirovecii cysts as the round dark purple spots.)
Blood should be collected to determine the serum concentrations of immunoglobulin G (IgG), IgM, and IgA IgG concentrations may be expected to be significantly low in pneumocystis-affected dogs, and IgM concentrations may be significantly high in affected dogs. See this 2006 study report. Decreased arterial oxygen tension is a recognized feature of the disease. See this April 1997 report.
Identification of pneumocystis by DNA analysis may also be performed. See this June 2001 report.
Given the possible inconclusive diagnosis by either BAL or needle biopsy, if the x-ray shows a generalized interstitial lung pattern and there is no obvious signs of cardiac failure (which otherwise could explain the rapid breathing and rapid heart rate), the examining veterinarian should be alert to the possibility of pneumocystis pneumonia. See this 1997 report.
In this March 2022 article, the authors gave this full definition of PCP:
"In order for a patient to have Pneumocystis pneumonia (PCP), all the following criteria must be present: (i) a consistent signalment, history and physical findings, often including key breed associations (e.g., CKCS), possible immunosuppression and a history of chronic progressive dyspnoea/polypnoea with non-productive coughing (ii) chest radiographs demonstrating a heavy diffuse interstitial pattern (bordering on an alveolar pattern), often accompanied by right side heart enlargement (cor pulmonale) and echocardiographic evidence for pulmonary hypertension, with chest CT showing abundant ground glass opacities (iii) representative BALF specimen containing Pneumocystis ascii (cysts) or trophic forms (zoites) and/or qPCR [quantitative polymerase chain reaction] positive for P. canis DNA with a CT below a defined cut-off, perhaps 26 (iv) unambiguous improvement in clinical status and radiological findings after treatment using trimethoprim sulpmethoxazole (often in concert with corticosteroids) and sometimes additional specific drugs directed against Pneumocystis."
RETURN TO TOP
Treatment
If the pneumocystis pneumonia is diagnosed at an early-enough stage, certain antibiotics have been effective in eliminating the spread of the fungus. A combination of trimethoprim and sulfamethoxazole ((Bactrim, Tribrissen, Di-Biotic, Borgal) has been a successful treatment, as has pentamidine isethionate (pentam 300).
Amphotericin B can be effective in killing the fungus, but is quite toxic and must be administered while the dog is on IV fluids to flush the kidneys. Other drugs that have been used include carbutamide, trimetrexate, and combinations of clindamycin, primaquine, dapsone, and trimethoprim.
Imidazole antifungal agents (itraconazole, fluconazole, ketoconazole, miconazole) have not proven effective in laboratory tests.
Additional therapies may include oxygen, mucolytics, bronchodilators, nebulization, and discontinuation of immunosuppressive medications.
Immunosuppression therapy (i.e., glucocorticoids) is not recommended. The use of immunosuppressive therapy in veterinary medicine may increase the prevalence of this condition. See this 1997 report.
In a March 2025 article, a 16-month-old cavalier King Charles spaniel with a history of progressive rapid respiratory rate (tachypnea), increased respiratory effort, and weight loss that had failed to respond to antimicrobial and antifungal treatments. The dog was diagnosed with pneumocystis pneumonia by polymerase chain reaction performed from an oropharyngeal swab. Secondary pulmonary hypertension was diagnosed with echocardiography. The dog was treated with a combination of trimethoprim-sulfonamide, an anti-inflammatory prednisone tapering course, and sildenafil with tapering course for pulmonary hypertension. The drugs completely resolved the clinical signs, and the treatment was ended.
RETURN TO TOP
Research News
March 2025:
Cavalier diagnosed with pneumocystis pneumonia is cured with
combined treatment of trimethoprim-sulfonamide, prednisone, and
sildenafil.
 In
a
March 2025 article, Missouri veterinary specialists Julie Nadeau,
Amber Graham (right), and Robyn Sherman report on the case
study of a 16-month-old cavalier King Charles spaniel with a history of
progressive rapid respiratory rate (tachypnea), increased respiratory
effort, and weight loss that had failed to respond to antimicrobial and
antifungal treatments. The dog was diagnosed with pneumocystis pneumonia
by polymerase chain reaction performed from an oropharyngeal swab.
Secondary pulmonary hypertension was diagnosed with echocardiography.
The dog was treated with a combination of trimethoprim-sulfonamide, an
anti-inflammatory prednisone tapering course, and sildenafil with
tapering course for pulmonary hypertension. The drugs completely
resolved the clinical signs, and the treatment was ended. The clinicians
reported that this is the first case report documenting pneumocystis
pneumonia diagnosed via oropharyngeal swab.
In
a
March 2025 article, Missouri veterinary specialists Julie Nadeau,
Amber Graham (right), and Robyn Sherman report on the case
study of a 16-month-old cavalier King Charles spaniel with a history of
progressive rapid respiratory rate (tachypnea), increased respiratory
effort, and weight loss that had failed to respond to antimicrobial and
antifungal treatments. The dog was diagnosed with pneumocystis pneumonia
by polymerase chain reaction performed from an oropharyngeal swab.
Secondary pulmonary hypertension was diagnosed with echocardiography.
The dog was treated with a combination of trimethoprim-sulfonamide, an
anti-inflammatory prednisone tapering course, and sildenafil with
tapering course for pulmonary hypertension. The drugs completely
resolved the clinical signs, and the treatment was ended. The clinicians
reported that this is the first case report documenting pneumocystis
pneumonia diagnosed via oropharyngeal swab.
March 2024:
Mutation of the CARMIL2 gene in cavaliers may cause the breed's
high percentage of Pneumocystis pneumonia.
 In a
March 2024 article, an international team of researchers (Emily L.
Coffey [right], Liang Ma, Ousmane H. Cissé, Joseph A. Kovacs, Katie M.
Minor, Antti Sukura, Patrizia Danesi, Steven G. Friedenberg, Jonah N.
Cullen, Christiane Weissenbacher-Lang, Julie C. Nadeau, Amber M. Graham,
Martin N. Granick, Natalie K. Branson, Kyle C. Branson, Barbara Blasi,
Casandra M. Jacobs, Eva Furrow) examined the DNA of 126 cavalier King
Charles spaniels and 15 dogs of other breeds to determine if an
immunodeficiency in cavaliers due to a mutation of the CARMIL2 gene made
the breed predisposed to Pneumocystis pneumonia (PCP) infections.
Previous research [see
this January 1996 article and
this March 2021
article] into the whole genome sequencing of a CKCS diagnosed with PCP
identified a variant of the CARMIL2 gene, which consists of 1,394 amino
acids. CARMIL2 deficiencies have been found to be a potential underlying
risk factor for PCP and other recurrent pneumonia in humans. The result
was that the researchers identified 2 PCP-affected cavaliers and one
CKCS infected with Bordetella pneumonia, all with a CARMIL2 variant.
These 3 dogs also suffered from non-respiratory clinical signs that
match CARMIL2 immunodeficiencies in humans. They recommend consideration
of the genetic testing of CKCSs for the CARMIL2 variant to aid in
clinical diagnosis of a primary immunodeficiency and guide breeding
practices, thereby reducing the frequency of this immunodeficiency in
the breed.
In a
March 2024 article, an international team of researchers (Emily L.
Coffey [right], Liang Ma, Ousmane H. Cissé, Joseph A. Kovacs, Katie M.
Minor, Antti Sukura, Patrizia Danesi, Steven G. Friedenberg, Jonah N.
Cullen, Christiane Weissenbacher-Lang, Julie C. Nadeau, Amber M. Graham,
Martin N. Granick, Natalie K. Branson, Kyle C. Branson, Barbara Blasi,
Casandra M. Jacobs, Eva Furrow) examined the DNA of 126 cavalier King
Charles spaniels and 15 dogs of other breeds to determine if an
immunodeficiency in cavaliers due to a mutation of the CARMIL2 gene made
the breed predisposed to Pneumocystis pneumonia (PCP) infections.
Previous research [see
this January 1996 article and
this March 2021
article] into the whole genome sequencing of a CKCS diagnosed with PCP
identified a variant of the CARMIL2 gene, which consists of 1,394 amino
acids. CARMIL2 deficiencies have been found to be a potential underlying
risk factor for PCP and other recurrent pneumonia in humans. The result
was that the researchers identified 2 PCP-affected cavaliers and one
CKCS infected with Bordetella pneumonia, all with a CARMIL2 variant.
These 3 dogs also suffered from non-respiratory clinical signs that
match CARMIL2 immunodeficiencies in humans. They recommend consideration
of the genetic testing of CKCSs for the CARMIL2 variant to aid in
clinical diagnosis of a primary immunodeficiency and guide breeding
practices, thereby reducing the frequency of this immunodeficiency in
the breed.
December 2023:
US clinicians report a thorough case study of pneumocystis
pneumonia in a cavalier.
 In
a December 2023 article
, US clinicians Brandon Verkinderen and Lisa M. Pohlman (right)
report a case study in Kansas of a 2-year-old cavalier King Charles
spaniel with progressively increased respiratory effort, up to 120
breaths per minute. Diagnosis is obtained by x-rays revealing a diffuse
mixed bronchial and interstitial pattern most consistent with an
infectious cause, and obtaining a bronchoalveolar lavage (BAL) sample
showing neutrophils, macrophages, and trophozoites. Treatment consisted
of sulfadiazine/trimethoprim for 21 days, dexamethasone for 3 days, and
theophylline for 14 days. Trazodone as needed for 14 days was
administered for sedation during the treatment period. This report is
particularly thorough and informative.
In
a December 2023 article
, US clinicians Brandon Verkinderen and Lisa M. Pohlman (right)
report a case study in Kansas of a 2-year-old cavalier King Charles
spaniel with progressively increased respiratory effort, up to 120
breaths per minute. Diagnosis is obtained by x-rays revealing a diffuse
mixed bronchial and interstitial pattern most consistent with an
infectious cause, and obtaining a bronchoalveolar lavage (BAL) sample
showing neutrophils, macrophages, and trophozoites. Treatment consisted
of sulfadiazine/trimethoprim for 21 days, dexamethasone for 3 days, and
theophylline for 14 days. Trazodone as needed for 14 days was
administered for sedation during the treatment period. This report is
particularly thorough and informative.
March 2022:
Italian study confirms that cavaliers are at increased risk for
pneumocystis pneumonia.
 In a
March 2022 article, a team of Italian and Australian veterinary
researchers (Patrizia Danesi [right], Matteo Petini, Christian Falcaro, Michela
Bertola, Elisa Mazzotta, Tommaso Furlanello, Mark Krockenberger, Richard
Malik) examined the bronchoalveolar lavage fluid (BALF) specimens of 255
dogs with respiratory distress and/or chronic cough, including 185
purebreds, of which ten were cavalier King Charles spaniels, the second
most common breed in this study. Two of the CKCSs (9%) tested positive
for DNA of the Pneumocystis fungus, among only 22 dogs overall. The
authors also provided this definition of PCP:
In a
March 2022 article, a team of Italian and Australian veterinary
researchers (Patrizia Danesi [right], Matteo Petini, Christian Falcaro, Michela
Bertola, Elisa Mazzotta, Tommaso Furlanello, Mark Krockenberger, Richard
Malik) examined the bronchoalveolar lavage fluid (BALF) specimens of 255
dogs with respiratory distress and/or chronic cough, including 185
purebreds, of which ten were cavalier King Charles spaniels, the second
most common breed in this study. Two of the CKCSs (9%) tested positive
for DNA of the Pneumocystis fungus, among only 22 dogs overall. The
authors also provided this definition of PCP:
"In order for a patient to have Pneumocystis pneumonia (PCP), all the following criteria must be present: (i) a consistent signalment, history and physical findings, often including key breed associations (e.g., CKCS), possible immunosuppression and a history of chronic progressive dyspnoea/polypnoea with non-productive coughing (ii) chest radiographs demonstrating a heavy diffuse interstitial pattern (bordering on an alveolar pattern), often accompanied by right side heart enlargement (cor pulmonale) and echocardiographic evidence for pulmonary hypertension, with chest CT showing abundant ground glass opacities (iii) representative BALF specimen containing Pneumocystis ascii (cysts) or trophic forms (zoites) and/or qPCR [quantitative polymerase chain reaction] positive for P. canis DNA with a CT below a defined cut-off, perhaps 26 (iv) unambiguous improvement in clinical status and radiological findings after treatment using trimethoprim sulpmethoxazole (often in concert with corticosteroids) and sometimes additional specific drugs directed against Pneumocystis."
May 2019: 7-month old cavalier with chronic cough is diagnosed with pneumocystis pneumonia infection. In an April 2019 article, a team of Italian veterinarians (Matteo Petini, Tommaso Furlanello, Patrizia Danesi, Andrea Zoia) report on the diagnosis and treatment of a 7-month-old female cavalier King Charles spaniel with a chronic cough which had not responded to any conventional antibiotic treatments. X-rays did not indicate that pneumocystis pneumonia (PP) was involved. However, the dog's symptoms, medical history, pathology, and DNA examination (nested polymerase chain reaction) findings confirmed that PP fungus was the cause.
April 2019: Australian case study of non-cavalier suggests cancer drug toceranib may cause pneumocystis pneumonia. In a May 2019 article, a team of Australian clinicians (MP Best, SP Boyd, P Danesi) report a case study of a Maltese terrier-Papillon mix being treated with toceranib phosphate as immunomodulatory therapy following mast cell cancer surgery. The dog developed a pneumocystis infection which was successfully treated with Trimethoprim/ sulfadiazine and oral prednisolone after stopping the toceranib. They concluded that:
"This case report describes PCP as a complication of therapy for the first time in dogs. It also highlights the potential for opportunistic infections in dogs treated with long-term toceranib. This disease is rapidly fatal if untreated but has a characteristic presentation and clinicians administering toceranib should be vigilant for symptoms of PCP. Such vigilance is particularly rewarding in light of the potential for rapid disease resolution with appropriate therapy, as seen in this case."
March 2018:
US cavalier is diagnosed with pneumocystis pneumonia using
polymerase chain reaction (PCR) analysis.
 In
a
March 2018 article, board certified internal medicine specialists
Ayeley A. K. Okine (right) and Roger A. Hostutler diagnosed a
2-year-old Ohio USA cavalier King Charles spaniel with pneumocystis
pneumonia using polymerase chain reaction (PCR) analysis. IDEXX
Laboratories were also involved in the analysis. The dog's symptoms
included: persistent dyspnea, inappetence, and lethargy for two weeks,
high respiratory rate (140 bpm), no heart murmur; x-rays showed a
moderately diffuse interstitial lung pattern suggestive of interstitial
pneumonia or possibly pulmonary edema; the right heart was prominent,
and pulmonary artery enlargement was suspected. An echocardiogram
revealed trivial to mild mitral valve regurgitation with no left-sided
chamber enlargement, moderate enlargement of the right atrium and
ventricle with moderate tricuspid valve regurgitation, and a moderately
dilated pulmonary artery with severely increased pulmonary arterial
pressure. A bronchoalveolar lavage (BAL) procedure was performed,
showing mixed inflammation with cysts and trophozoites consistent with
pneumocystis. Pneumocystis infection was later confirmed with polymerase
chain reaction (PCR) analysis. This apparently is the first case of
canine pneumocystis pneumonia diagnosed with PCR from a BAL sample.
In
a
March 2018 article, board certified internal medicine specialists
Ayeley A. K. Okine (right) and Roger A. Hostutler diagnosed a
2-year-old Ohio USA cavalier King Charles spaniel with pneumocystis
pneumonia using polymerase chain reaction (PCR) analysis. IDEXX
Laboratories were also involved in the analysis. The dog's symptoms
included: persistent dyspnea, inappetence, and lethargy for two weeks,
high respiratory rate (140 bpm), no heart murmur; x-rays showed a
moderately diffuse interstitial lung pattern suggestive of interstitial
pneumonia or possibly pulmonary edema; the right heart was prominent,
and pulmonary artery enlargement was suspected. An echocardiogram
revealed trivial to mild mitral valve regurgitation with no left-sided
chamber enlargement, moderate enlargement of the right atrium and
ventricle with moderate tricuspid valve regurgitation, and a moderately
dilated pulmonary artery with severely increased pulmonary arterial
pressure. A bronchoalveolar lavage (BAL) procedure was performed,
showing mixed inflammation with cysts and trophozoites consistent with
pneumocystis. Pneumocystis infection was later confirmed with polymerase
chain reaction (PCR) analysis. This apparently is the first case of
canine pneumocystis pneumonia diagnosed with PCR from a BAL sample.
March 2018:
Computed tomography successfully diagnosed pneumocystis
carinii pneumonia in four cavaliers.
 In
a March 2018 article, UK
clinicians (Frederike Schiborra [right], C. J. Scudder, R. M.
Littler, C. R. Lamb, J. F. McConnell, T. W. Maddox) examined four
cavalier King Charles spaniels diagnosed with pneumocystis carinii
pneumonia. They used computed tomography (CT) to confirm the
diagnoses. They reported that:
In
a March 2018 article, UK
clinicians (Frederike Schiborra [right], C. J. Scudder, R. M.
Littler, C. R. Lamb, J. F. McConnell, T. W. Maddox) examined four
cavalier King Charles spaniels diagnosed with pneumocystis carinii
pneumonia. They used computed tomography (CT) to confirm the
diagnoses. They reported that:
"Thoracic CT revealed ground glass opacity of the pulmonary parenchyma with a diffuse or multifocal distribution. The severity of this pattern was variable. Less consistent imaging findings included parenchymal bands, bronchial dilation and signs consistent with pulmonary hypertension. Four dogs recovered well with treatment and there was resolution of CT abnormalities in all dogs with follow-up. "
 November
2017:
Austrian researchers suspect cavaliers may have an impaired
immunity to Pneumocystis infection. In a
November 2017 article in which a team of Austrian veterinarians
(Christiane Weissenbacher-Lang [right], Andrea
Fuchs-Baumgartinger, Abigail Guija-De-Arespacochaga, Andrea Klang,
Herbert Weissenböck, Frank Künzel) studied the case histories of 43 dogs
with Pneumocystis infection, including 16 cavalier King Charles
spaniels, they concluded that a breed predisposition for cavaliers is
evident and that an underlying heritable immunodeficiency in the breed
is suspected.
November
2017:
Austrian researchers suspect cavaliers may have an impaired
immunity to Pneumocystis infection. In a
November 2017 article in which a team of Austrian veterinarians
(Christiane Weissenbacher-Lang [right], Andrea
Fuchs-Baumgartinger, Abigail Guija-De-Arespacochaga, Andrea Klang,
Herbert Weissenböck, Frank Künzel) studied the case histories of 43 dogs
with Pneumocystis infection, including 16 cavalier King Charles
spaniels, they concluded that a breed predisposition for cavaliers is
evident and that an underlying heritable immunodeficiency in the breed
is suspected.
October 2012: UK/South African veterinary pathologist finds pneumocystis infection in a cavalier. In an October 2012 study, UK/South African veterinary pathologist Emma Scurrell reported identifying pneumocytis pneumonia in a 1-year-old cavalier King Charles spaniel showing symptoms of tachypnoea and dyspnoea.
April 2012: UK diagnostic lab identifies pneumocystis carinii pneumonia in a CKCS. In an April 2012 study, UK's Carmichael Torrance Veterinary Diagnostic Lab reported diagnosing pneumocystis carinii pneumonia in a 4 year old cavalier with symptoms of recurrent dyspnoea and tachypnoea and showed a generalized interstitial pattern on x-ray.
February 2012: UK diagnostic veterinary lab pneumocystis carinii pneumonia in a CKCS. In a February 2012 study, Richard Fox, veterinary pathologist at Abbey Veterinary Services, a UK diagnostic veterinary laboratory, diagnosed pneumocystis carinii pneumonia in a 6 year old cavalier King Charles spaniel with a recent history of increased respiration and a marked bilateral and diffuse interstitial pattern on its lung x-ray.
RETURN TO TOP
Related Links
RETURN TO TOP
Veterinary Resources
A retrospective study of diagnosis in 109 cases of canine lower respiratory disease. S. E. Brownlie. J. Sm. Anim. Pract. August 1990;31(8):371-376. Quote: Between 1983 and 1988, 109 cases of canine lower respiratory tract disease were examined and categorised according to clinical, radiographic and bronchoscopic findings and cytology of bronchial mucus. Non-specific chronic tracheobronchitis was diagnosed in 19 cases, bronchopneumonia (subacute or chronic) in 12 cases, bronchiectasis in 10 cases, parasitic bronchitis due to Oslerus osleri in 20 cases, eosinophilic bronchitis with or without bronchiectasis or alveolar infiltration in 25 cases, bronchial foreign bodies, mainly cereal ears, in 14 cases, primary neoplasia (adenocarcinomas) in six cases and miscellaneous disease in three cases. Features of these conditions are discussed. ... Chronic: Two young dogs, a seven-month-old shar pei and a 10-month-old cavalier King Charles spaniel, had skin disease which was identified as demodectic mange. The latter dog also had bilateral severe otitis externa and frequent diarrhoea, suggesting a possible immune deficiency. ... Radiographs showed patchy alveolar densities throughout the lung fields and an increased bronchial pattern. Cytology of bronchial mucus revealed many neutrophils, with mononuclear cells, epithelial cells and occasionally bacteria. Pasteurella, staphylococci and a-haemolytic streptococci were cultured from one dog, and a pure culture of Staphylococcus intermedius from another. The prognosis in this group of cases was poor. ... Parasitic bronchitis: Breeds affected by parasitic bronchitis: Cavalier King Charles spaniel 3. ... All cases stopped coughing except for one badly affected animal, a cavalier King Charles spaniel, which was endoscoped on four occasions. The results are shown in Table 3. Table 3: Cavalier King Charles spaniel, male two-and-a-half years. Duration of signs 18 months. Day 1: Massive nodules at tracheal bifurcation almost obliterating airway. Worms visible in nodules. Many larvae in tracheal mucus and faeces. Fenbendazole 50 mg/kg daily for 14 days. Day 16: Dog still wheezing and coughing. Nodules slightly flattened but similar to day 1 in appearance. Fenbendazole 50 mg/kg daily for 14 days. Day 47: Dog clinically better. Occasional cough. Several nodules still present but worms not visible No further treatment. Day 131: Dog well - no signs. Three tiny nodules still visible. Two larvae found in bronchial mucus. ... Miscellaneous: Three dogs were seen with severe pulmonary conditions causing dyspnoea and coughing. These were a young cavalier King Charles spaniel with pneumonia due to Pneumocystis carinii infection ... Although the aetiology of chronic bronchial disease may not always be ascertained, it is important to assign a dog to a diagnostic category so that the owner can be given a more accurate prognosis.
Pneumocystis Carinii Pneumonia in Dogs -- a Diagnostic Challenge. Antti Sukura, Seppo Saari, Anna-Kaisa Järvinen, Mats Olsson, Marjatta Kärkkäinen and Timo Ilvesniemi. J.Vet.Diagn.Invest. January 1996; doi: 10.1177/104063879600800124. Quote: "A Cavalier Ring Charles Spaniel (1.5 years, male) with respiratory signs unresponsive to therapy ... had suffered many problems during its first year, including tibial fracture, a large abscess in the stifle region, gastroenteritis, and erosive inflammation in the mouth and tongue. Erosive lesions were detected also at the beginning of the respiratory disease. The examination for canine distemper virus by immunofluorescence testing of cytological specimens had been negative. The dog had been vaccinated twice against distemper. Progressive respiratory signs had appeared 2 months prior to referral and included cough and dyspnea. The dog exhibited poor appetite and exercise intolerance. Therapy with antibiotics (amoxicillin clavulanic acid, tetracycline, cephalexin) produced no response. Some relief, especially at night, was obtained with low-dose corticosteroids (2.5 mg prednisolone/day for 1 month). The dog was afebrile and dyspneic with increased abdominal effort in respiration. Cyanosis became evident after slight exercise. Lung auscultation revealed respiratory crackles and wheezes. A soft murmur was auscultated on the left and right thorax. In thoracic radiographs diffuse interstitial and peribronchial densities were seen throughout the lungs, giving the impression of a reticular structure with micronodule formations. Chronic alveolar densities could be seen in all parts of the lungs. ... A diagnosis of P. carinii pneumonia was made on the basis of the preliminary results, and specific therapy with high dose (60 mg/kg/day) trimethoprim sulfonamide and folinic acid (1 mg/kg/day)11 was initiated, but the dog died on the same day the medication was instituted, and was sent to necropsy. A thorough necropsy showed the dog to be slightly emaciated, with all visible mucosal membranes cyanotic. All lymph nodes were atrophic and difficult to find; histopathologically they lacked germinal centers as well as paracortical lymphoid tissue. The architecture of the remaining structures was loose. The spleen was small and firm, showing histopathologically only a few follicular structures and periarterial lymphoid sheaths. The splenic trabeculae were prominent. In the heart, mild changes typical of endocardiosis were seen in the atrioventricular valves. The main gross lesions were associated with the lungs. The lungs were diffusely edematous, firm, and rubbery. The general color was brownish red, with diffuse yellowish-brown granular and patchy foci. The trachea and main bronchi were clean. A serous exudate in the distal bronchioli and interstitial tissue was easily detected on the cut surface of the lung. Formalin -fixed and paraffin-embedded lung-tissue specimens were stained with hematoxylin and eosin (HE), van Gieson, Gomori’s modification of Grocott’s methenamine silver staining (GMS), and immunohistochemically with the avidin-biotin peroxidase method, with the primary antibody being P. carinii-specific monoclonal antibody (DMo).h This antibody is known to stain both cyst and trophozoite stages of human-origin organisms.30 The lung showed changes typical for diffuse interstitial pneumonia; in some areas only minimal inflammation was present, with the number of inflammatory cells generally low, consisting mainly of macrophages with a smaller number of polymorphonuclear neutrophils and lymphocytes."
Pneumocystis carinii pneumonia in two Cavalier King Charles spaniels. Ramsey IK, Foster A, McKay J, Herrtage ME. Vet Rec. 1997 Apr 5;140(14):372-373. Quote: "This report describes two clinical cases of pneumonia in Cavalier King Charles spaniels in which large numbers of P carinii cysts were identified at postmortem examination. The first dog was a three-year-old neutered female that presented with a six week history of increasing respiratory distress. Treatment with various antibiotics, etamiphylline and glucocorticoids by the referring veterinary surgeon had been unsuccessful. On clinical examination the dog was found to be thin and tachypnoeic (100 to 160 breaths/minute). Despite this severe respiratory distress the dog was only slightly depressed. Rectal temperature was normal and the submandibular lymph nodes were slightly enlarged. On thoracic auscultation the lung sounds were diffusely increased and there was no cardiac murmur. Haematology demonstrated increased numbers of neutrophils, monocytes, eosinophils and a mild thrombocytopenia. Routine biochemistry was normal. Arterial blood gas analysis demonstrated reduced oxygen tension (59 mmHg) and haemoglobin saturation (91 per cent). Thoracic radiography showed a severe generalised interstitial lung pattern with patches of a superimposed alveolar pattern. The cardiac silhouette was of normal size and shape. Bronchoscopy under general anaesthesia was unremarkable. Cytology and bacterial culture of a bronchoalveolar lavage were unhelpful. The dog's condition progressively deteriorated and it was euthanased two months after first developing signs of respiratory disease. The second case was a 17-month-old entire female Cavalier King Charles spaniel that was presented with a two week history of progressive dyspnoea and occasional cyanosis. Clinical examination revealed tachypnoea (160 breaths/minute), tachycardia (170 beats/minute), slight cyanosis, a normal rectal temperature and harsh lung sounds over all lung fields. The dog was not depressed despite the severe clinical signs and no heart murmur was heard. Haematology demonstrated neutrophilia, monocytosis and eosinophilia. Routine biochemistry was normal. Arterial blood gas analysis demonstrated reduced oxygen tension (46.5 mmHg) and haemoglobin saturation (81 per cent). No antibodies to Toxoplasma gondii or Aspergillus species were detected on serological examination. Faecal examination did not demonstrate any lungworm larvae. A thoracic radiograph demonstrated an increased interstitial pattern and a pneumomediastinum. A prominent pulmonary artery segment was noted on the dorsoventral projection. Treatment with frusemide, enrofloxacin and anti-inflammatory doses of prednisolone was initially successful in reducing the respiratory rate. Bronchoscopy and bronchoalveolar lavage were then performed under general anaesthesia. Cytological examination of the lavage fluid did not identify a cause for the dog's respiratory distress. A fine needle aspirate of the right lung was non-diagnostic. Following this procedure the dog developed a pneumothorax which resolved following drainage. The dog's clinical condition remained stable for a few weeks but she died at home 10 weeks after the initial development of clinical signs. On postmortem examination both dogs had diffuse consolidation of the lungs which exuded foam from their cut surfaces. In the first case there were also multiple white foci, which were 1 to 2 mm in diameter, present over all the lobes and the bronchial lymph nodes were enlarged. Both cases showed similar histological changes, but the changes were more pronounced in the first case. ... The clinical signs of tachypnoea without pyrexia in a young dog with a generalised interstitial lung pattern and without obvious signs suggestive of cardiac failure should alert the clinician to the possibility of pneumocystic pneumonia. The decreased arterial oxygen tension seen in both cases is a recognised feature of the disease in humans and has been reported in other canine patients. Definitive diagnosis in the live patient can be difficult as bronchoalveolar lavages may be unhelpful (Farrow and others 1972). Fine needle lung aspirates are more reliable but there is an increased risk of complications, especially in animals whose respiratory function is already severely compromised. More invasive techniques, such as percutaneous lung biopsies and open lung biopsies, would be expected to carry even more risks. Data from human studies suggest that untreated pneumocystic pneumonia is uniformly fatal; however, the mortality rate in treated humans is 25 per cent. Trimethoprim-sulphamethoxazole appears to be the treatment of choice in canine patients. Short-term improvements have also been seen in response to glucocorticoid therapy. Given the role of immunosuppression in the pathogenesis of the disease in humans this therapeutic approach is not recommended in confirmed cases. ... The expanding use of immunosuppressive therapy in veterinary medicine may increase the prevalence of this condition. ... This has led to speculation that there may be an inherited immunodeficiency in this breed, although the affected dogs can make a full recovery and do not show clinical signs of other opportunistic infections. ... It is possible that there is a breedspecific factor that predisposes Cavalier King Charles spaniels in the UK to the development of this condition."
Case II - PM91-067 (AFIP 2642601). AFIP Wednesday Slide Conference - No. 27. April 21, 1999. Conference Moderator: LTC A. Peter Vogel. Contributor: Department of Veterinary Pathology, University of Liverpool. Quote: "Signalment: Two-year-old, male, Cavalier King Charles Spaniel, canine. History: There was tachypnea of two months duration and occasional diarrhea. The referring veterinarian treated the dog with antibiotics and steroids, but there was no response. The dog was referred to the Small Animal Hospital, University of Liverpool. On clinical examination, the dog was non-febrile, cyanotic, tachypneic, tachycardic, and had prominent mesenteric lymph nodes. Radiographs demonstrated marked interstitial pattern in lungs, an enlarged liver, and possibly enlarged sublumbar lymph nodes. The other lymph nodes were unremarkable. Gross Pathology: Respiratory System: The external nares, frontal sinuses and pharynx were unremarkable. The larynx, and especially trachea and bronchi, contained pale, stable foam and were lined by pale epithelium. The lungs collapsed partially on opening the chest. The cut surfaces of all lobes were grey-pink, firm, poorly-aerated, and exuded abundant fluid. The pleural surfaces were smooth and glistening without excess fluid. The macroscopic diagnosis was pulmonary consolidation. ... Contributor's Diagnosis and Comments: Lung: Chronic active interstitial pneumonia with myriad ring-shaped organisms typical of cyst forms of Pneumocystis carinii, Cavalier King Charles Spaniel, canine. Autolytic changes include detachment of airway epithelial cells. There is abundant eosinophilic, foamy, granular contents in airway lumina in which a few cells and faintly stained ring structures are also present. There are inflammatory cells (mostly lymphocytes and plasma cells) and patchy fibroplasia in alveolar septa. There is variable hyperplasia of type II pneumocytes. Methenamine silver staining reveals myriad ring-shaped organisms typical of cyst forms of Pneumocystis carinii in airway and alveolar lumina. This Cavalier King Charles Spaniel had advanced chronic active interstitial pneumonia in which organisms with morphological and staining characteristics of cyst forms of Pneumocystis carinii are identified. ... AFIP Diagnosis: Lung: Pneumonia, interstitial, chronic, diffuse, mild, with abundant alveolar and intra-airway eosinophilic flocculent material (atypical fungi), Cavalier King Charles Spaniel, etiology consistent with Pneumocystis carinii."
Pneumocystis carinii pneumonia in a Cavalier King Charles Spaniel. Hagiwara Y, Fujiwara S, Takai H, Ohno K, Masuda K, Furuta T, Nakayama H, Doi K, Tsujimoto H. J Vet Med Sci. 2001 Mar;63(3):349-51. Quote: "Pneumocystis carinii pneumonia was diagnosed by postmortem examination of a one-year-old Cavalier King Charles Spaniel with four-week history of dyspnea. Cytologic and histologic examination of lung tissues revealed numerous P. carinii trophozoites and cysts, and P. carinii specific DNA was detected by polymerase chain reaction. The dog showed hypogammagloblinemia and extremely low levels of serum IgG. It was considered that P. carinii pneumonia in this case was associated with an immunodeficient condition which has already been reported in Miniature Dachshunds."
DNA Analysis of Pneumocystis Infecting a Cavalier King Charles Spaniel. Kate English, Sarah E. Peters, Duncan J. Maskell, Margaret E. Collins. J. Eukaryotic Microbiology; June 2001;48(s1):106s. Quote: "Lung tissue was obtained from a 20-month old entire female Cavalier King Charles Spaniel which had been diagnosed with PCP post mortem by identification of Pneumocystis cysts. ... RESULTS AND DISCUSSION: The product of the PCR reaction was approximately 350 base pairs, similar in size to the PCR product generated from a positive control P. carinii from rat, and was consistent with amplification of a Pneumocystis-specific product. On sequencing seven clones of the PCR products two distinct DNA sequences were observed. Five clones gave Type A, and two Type B. A representative of each sequence type was sequenced on both strands to verify the data. The two sequences were shown to have 86.9% identity when compared to each other ... A FASTA search of the European Molecular Biology Laboratory Database found greatest identity with mt LSU rRNA Pneumocystis sequences derived from other host species. The identity with the sequence of Pneunocystis derived from other host species ranged from 87%-73% in the region compared. We have therefore shown that this dog was infected with a genetically distinct form of Pneumocystis and propose that Pneumocystis infecting a canine host be referred to as Pneumocystis canis. It is also proposed that the two forms be temporarily designated Type A and Type B while awaiting furthcr clarification of their relationship."
Immunoglobulin Deficiency in Cavalier King Charles Spaniels with Pneumocystis Pneumonia. P.J. Watson, P. Wotton, J. Eastwood, S.T. Swift, B. Jones, and M.J. Day. J Vet Intern Med 2006;20:523–527. Quote: "Serum concentrations of immunoglobulin G (IgG), IgM, and IgA were measured in 9 Cavalier King Charles Spaniels with pneumonia caused by Pneumocystis sp that were examined at 4 veterinary surgeries in the United Kingdom (UK) between September 2001 and November 2002. Pneumocystis pneumonia was confirmed in all dogs by visualization of the organism in bronchoalveolar lavage fluid or a transthoracic lung aspirate. Two dogs had a history of demodicosis. Immunoglobulin concentrations also were measured in breed-and age-matched dogs sampled over the same period. IgG concentrations were significantly (P 5 .000) lower in the affected dogs (median 3.2 mg/mL) than in the control dogs (median 8.5 mg/mL). IgM concentrations were significantly (P 5 .002) higher in the affected dogs (median 1.95 mg/mL) than in the control dogs (median 1.12 mg/mL). One affected dog had no change in IgG concentration more than 3 months after resolution of infection or vaccination, but did have reduction in IgM concentration after resolution of infection and vaccination. Control dogs had low serum IgG and IgM concentrations, compared with the reference interval for all dogs. Lymphocyte count in blood was normal or high in 7 of 8 affected dogs. The results of this study suggest that there is a defect in immunity in Cavalier King Charles Spaniels that underlies the susceptibility of these dogs to pneumocystosis. Further studies are indicated to elucidate the mechanisms behind the defect, the prevalence within the breed, and the potential mode of inheritance of the problem."
Pneumocystis pneumonia in two Cavalier King Charles Spaniel littermates. Meffert, F. J. Australian Vet. Practitioner 2009; 39(1):2-2...9. Quote: "Pneumocystis pneumonia was diagnosed in two Cavalier King Charles Spaniel littermates with a chronic history of intermittent respiratory signs including tachypnoea, coughing and dyspnoea. Thoracic radiographs showed a diffuse interstitial pattern. Pneumocystis organisms were identified on cytological and histopathological examination of lung tissue at necropsy (of the first dog) and on pre mortem cytological examination of bronchial secretions from a second dog. The first dog was euthanised due to rapid deterioration prior to diagnosis. The second dog developed megaoesophagus two months after diagnosis of pneumocystis pneumonia and was euthanised due to persistent regurgitation. To the author's knowledge, this is the first report of pneumocystis pneumonia in Cavalier King Charles Spaniel littermates and provides further support for an underlying inheritable immunodeficiency in this breed."
Underlying diseases in dogs referred to a veterinary teaching hospital because of dyspnea: 229 cases (2003–2007). Sonja Fonfara, Lourdes de la Heras Alegret, Alexander J. German, Laura Blackwood, Joanna Dukes-McEwan, P-J. M. Noble, Rachel D. Burrow. JAVMA. November 2011; doi:10.2460/javma.239.9.1219. Quote: Objective: To identify the most frequent underlying diseases in dogs examined because of dyspnea and determine whether signalment, clinical signs, and duration of clinical signs might help guide assessment of the underlying condition and prognosis. Design: Retrospective case series. Animals: 229 dogs with dyspnea. ... A range of breeds were included, with Bulldogs (n = 22), Labrador Retrievers (20), mixed breeds (19), and Cavalier King Charles Spaniels (19) being most common. ... Procedures: Case records of dogs referred for dyspnea were reviewed and grouped according to location or etiology (upper airway, lower respiratory tract, pleural space, cardiac diseases, or obesity and stress). Signalment, clinical signs at initial examination, treatment, and survival time were analyzed. Results: Upper airway (n = 74 [32%]) and lower respiratory tract (76 [33%]) disease were the most common diagnoses, followed by pleural space (44 [19%]) and cardiac (27 [12%]) diseases. Dogs with upper airway and pleural space disease were significantly younger than dogs with lower respiratory tract and cardiac diseases. Dogs with lower respiratory tract and associated systemic diseases were significantly less likely to be discharged from the hospital. ... Two of the dogs with bacterial bronchopneumonia were Cavalier King Charles Spaniels and were diagnosed with Pneumocystis carinii infection. ... Dogs with diseases that were treated surgically had a significantly better outcome than did medically treated patients, which were significantly more likely to be examined on an emergency basis with short duration of clinical signs. Conclusions and Clinical Relevance: In dogs examined because of dyspnea, young dogs may be examined more frequently with breed-associated upper respiratory tract obstruction or pleural space disease after trauma, whereas older dogs may be seen more commonly with progressive lower respiratory tract or acquired cardiac diseases. Nontraumatic acute onset dyspnea is often associated with a poor prognosis, but stabilization, especially in patients with cardiac disease, is possible. Obesity can be an important contributing or exacerbating factor in dyspneic dogs.
A Case of Suspected Pneumocystis carinii Pneumonia in a Cavalier King
Charles Spaniel. Richard Fox. Abbey Vet. Serv. Feb. 2012.
Quote: "A male neutered 6-years-old Cavalier King Charles Spaniel
presented with a 5 day history of increased respiratory effort. Radiographic
examination revealed a marked bilateral and diffuse interstitial pattern. The
dog was anaethetised and a bronchoalveolar lavage was performed from both the
right and left lung fields. The sample was sent for
 cytological
examination. Cytospin and direct preparations were made of both samples and
stained with a Rapid Romanowsky Stain. Degenerate neutrophils , small
lymphocytes and infrequent erythrocytes (see photo at right) were
prevelant. There were also several extracellular colonies of monomorphic short
bacilliary bacteria exhibiting bipolar staining. Occasional neutrophils appeared
to contain similar bacteria within their cytoplasm. The smear of BAL fluid from
the right side revealed a more cellular harvest than that of the left side but
its cellularity was qualitatively similar. However, there were multiple
organisms present dissimilar to the bacteria previously noted. A few
extracellular basophilic bodies were present. Most were approximately 3-4 um in
diameter, homogenous basophilic staining associated with a background of
flocculant basophilic material. Infrequently however there were similarly sized
organisms with 8 spindle shaped deeply basophilic structures (8-10 um diameter).
These organisms, given the breed and presence of numerous foamy macrophages were
considered compatible with Pneumocystis trophozoites. Also a few septate fungal
hyphae and pleomorphic bacteria were noted in the BAL from the right side. ...
Numerous darkly staining spherical organisms (in addition to the fungal hyphae)
were noted. Closer examination of less darkly stained structures reveiled a
typical yeast like structure. Pneumocystoisis was then suspected but identifying
a convenient laboratory which would perform PCR testing was not possible at the
time of diagnosis. ... CKCS and Miniature Dachshunds appear to
be predisposed to infection due to a suspected immunodeficient condition. ...
The diagnosis is made by identifying the fungi in histologic sections. ...
Pneumocystis cannot be cultured using conventional techniques, but novel cell
culture systems have recently been described. A PCR test has been developed
however."
cytological
examination. Cytospin and direct preparations were made of both samples and
stained with a Rapid Romanowsky Stain. Degenerate neutrophils , small
lymphocytes and infrequent erythrocytes (see photo at right) were
prevelant. There were also several extracellular colonies of monomorphic short
bacilliary bacteria exhibiting bipolar staining. Occasional neutrophils appeared
to contain similar bacteria within their cytoplasm. The smear of BAL fluid from
the right side revealed a more cellular harvest than that of the left side but
its cellularity was qualitatively similar. However, there were multiple
organisms present dissimilar to the bacteria previously noted. A few
extracellular basophilic bodies were present. Most were approximately 3-4 um in
diameter, homogenous basophilic staining associated with a background of
flocculant basophilic material. Infrequently however there were similarly sized
organisms with 8 spindle shaped deeply basophilic structures (8-10 um diameter).
These organisms, given the breed and presence of numerous foamy macrophages were
considered compatible with Pneumocystis trophozoites. Also a few septate fungal
hyphae and pleomorphic bacteria were noted in the BAL from the right side. ...
Numerous darkly staining spherical organisms (in addition to the fungal hyphae)
were noted. Closer examination of less darkly stained structures reveiled a
typical yeast like structure. Pneumocystoisis was then suspected but identifying
a convenient laboratory which would perform PCR testing was not possible at the
time of diagnosis. ... CKCS and Miniature Dachshunds appear to
be predisposed to infection due to a suspected immunodeficient condition. ...
The diagnosis is made by identifying the fungi in histologic sections. ...
Pneumocystis cannot be cultured using conventional techniques, but novel cell
culture systems have recently been described. A PCR test has been developed
however."
A case of Pneumocystis carinii pneumonia in a 4 year old Cavalier King Charles Spaniel. Carmichael Torrance Vet. Diagnostic Lab. April 2012. Quote: "The dog had presented with recurrent dyspnoea and tachypnoea and showed a generalized interstitial pattern on radiographs. A few small round granular structures are found in a cytospin preparation from a BAL, consistent with Pneumocystis Carinii. This may be associated with an immunodeficient condition which has already been reported in Miniature Dachshunds, and assessment of the immunoglobulins (IgA, IgM and IgG) is advisable in these cases. PCR is also available, although this is usually carried out on lung tissue rather than washing fluid and false negative results may be possible."
 Pneumocystis
infection in a Cavalier King Charles Spaniel. Emma
Scurrell. CytoPath Vet. Path. Lab. Oct. 2012. Quote: "A 1-year-old male
CKCS presented for tachypnoea and dyspnoea. Radiographs revealed an
interstitial lung pattern. The rectal temperature was normal. A bronchoalveolar
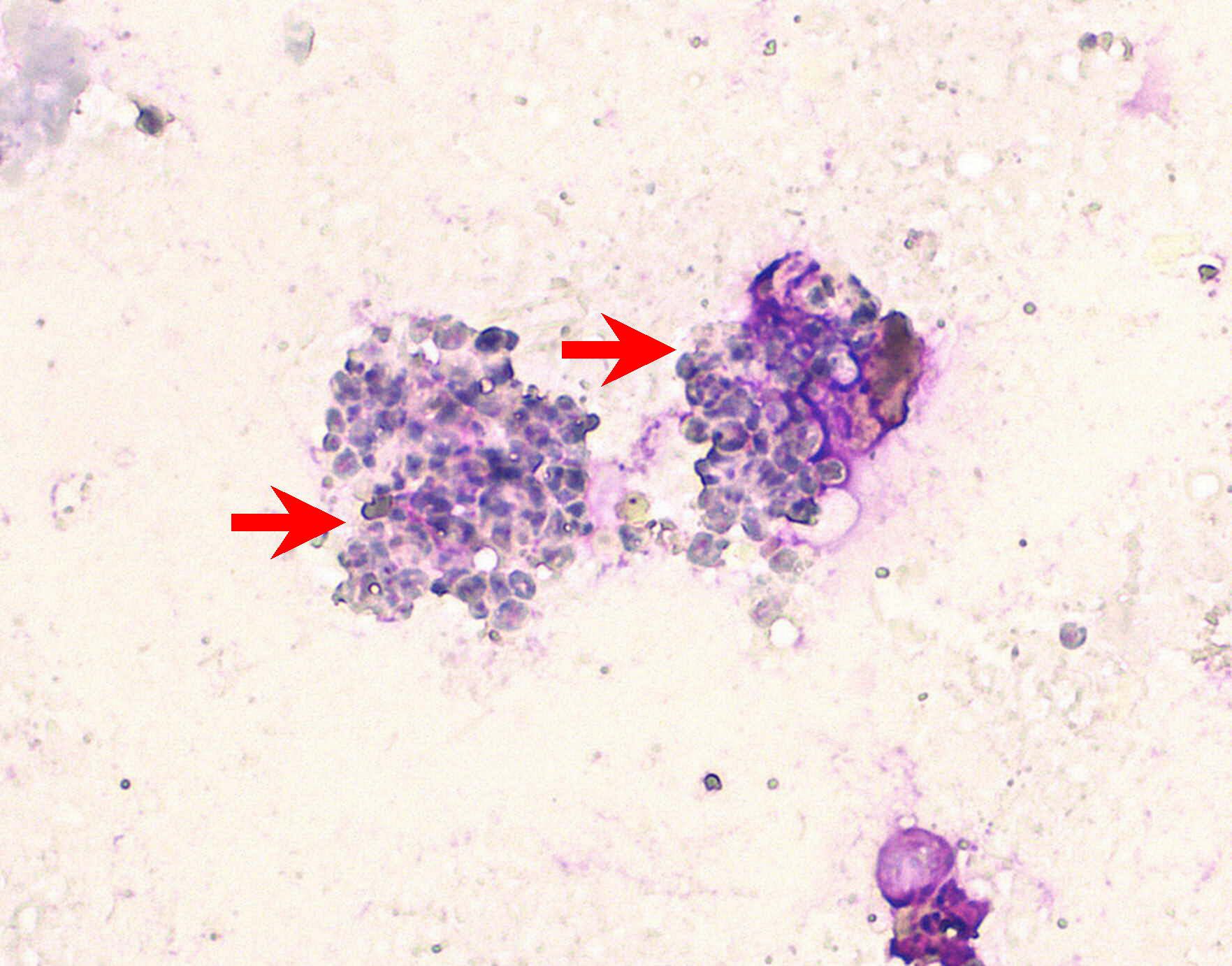
lavage (BAL) was performed. Fig 1 (right). Cytological findings
revealed low numbers of neutrophils and macrophages and large numbers of extra-
and intracellular 4-5um organisms typical of Pneumocystis spp. The red arrows
point to two macrophages which are distended by the small fungal bodies (stained
with modified Wrights-Giemsa). Final Diagnosis: Pneumocytis pneumonia.
Discussion: Pneumocystis is an opportunistic fungal pathogen affecting humans
and animals with impaired immunity. The entire life cycle is in the lungs and
lesions are usually limited to the lungs. Any breed of dog can potentially be
affected however Miniature Dachshunds and Cavalier King Charles Spaniels
are predisposed, suspected to be associated with underlying immunodeficiency.
Affected CKCSs have been shown to have decreased levels of IgG
compared to control dogs. Diagnosis is usually made on direct visualisation of
the organisms in BAL fluid or in a transthoracic lung aspirate. The organism
will not culture using conventional techniques."
Pneumocystis
infection in a Cavalier King Charles Spaniel. Emma
Scurrell. CytoPath Vet. Path. Lab. Oct. 2012. Quote: "A 1-year-old male
CKCS presented for tachypnoea and dyspnoea. Radiographs revealed an
interstitial lung pattern. The rectal temperature was normal. A bronchoalveolar
lavage (BAL) was performed. Fig 1 (right). Cytological findings
revealed low numbers of neutrophils and macrophages and large numbers of extra-
and intracellular 4-5um organisms typical of Pneumocystis spp. The red arrows
point to two macrophages which are distended by the small fungal bodies (stained
with modified Wrights-Giemsa). Final Diagnosis: Pneumocytis pneumonia.
Discussion: Pneumocystis is an opportunistic fungal pathogen affecting humans
and animals with impaired immunity. The entire life cycle is in the lungs and
lesions are usually limited to the lungs. Any breed of dog can potentially be
affected however Miniature Dachshunds and Cavalier King Charles Spaniels
are predisposed, suspected to be associated with underlying immunodeficiency.
Affected CKCSs have been shown to have decreased levels of IgG
compared to control dogs. Diagnosis is usually made on direct visualisation of
the organisms in BAL fluid or in a transthoracic lung aspirate. The organism
will not culture using conventional techniques."
Finding your Way Through Pneumocystis Sequences in the NCBI Gene Database. Christiane Weissenbacher-Lang, Nora Nedorost, Herbert Weissenböck. J. Eukaryotic Microbiology. Sept. 2014;61(5):537-555. Quote: "Pneumocystis sequences can be downloaded from GenBank for purposes as primer/probe design or phylogenetic studies. Due to changes in nomenclature and assignment, available sequences are presented with a variety of inhomogeneous information, which renders practical utilization difficult. The aim of this study was the descriptive evaluation of different parameters of 532 Pneumocystis sequences of mitochondrial and ribosomal origin downloaded from GenBank with regard to completeness and information content. Pneumocystis sequences were characterized by up to four different names. Official changes in nomenclature have only been partly implemented and the usage of the 'forma specialis', a special feature of Pneumocystis, has only been established fragmentary in the database. Hints for a mitochondrial or ribosomal genomic origin could be found, but can easily be overlooked, which renders the download of wrong reference material possible. The specification of the host was either not available or variable regarding the used language and the localization of this information in the title or several subtitles, which limits their applicability in phylogenetic studies. Declaration of products and geographic origin was incomplete."
Pneumocystis canis pneumonia in dogs. Elizabeth Ralph, George Reppas, Catriona Halliday, Mark Krockenberger, Richard Malik. Microbiology Australia. March 2015; 10.1071/MA15026:A-D. Quote: Pneumocystis canis is a potential cause of life-threatening interstitial fungal pneumonia in dogs. It is seen almost exclusively in two canine breeds, miniature Dachshunds and Cavalier King Charles Spaniels (CKCS). Historically, Australian veterinarians had a key role in the documentation of this entity and its conspicuous breed associations. Affected Dachshunds and CKCS are likely to have an inherited immunodeficiency that predisposes them to infection with this commensal organism of the respiratory tract and pharynx. A high index of suspicion is required to make a timely diagnosis and save affected patients, as these dogs cope poorly with anaesthesia and other measures to procure the specimens required to make a definitive diagnosis. Possible co-infection with Bordetella bronchiseptica must be considered when determining antimicrobial strategies. Affected dogs occasionally have a previous or concurrent history of generalised demodicosis. With early intervention, affected dogs can be saved, although some require life-long therapy to prevent recurrence. The future challenge is to develop fast molecular techniques to diagnose P. canis pneumonia (PCP) and to determine the underlying immune defect in over-represented breeds through the rapidly advancing field of canine genomics.
Molecular diagnosis of Pneumocystis pneumonia in dogs. Patrizia Danesi, Silvia Ravagnan, Lynelle R. Johnson, Tommaso Furlanello, Adelaide Milani, Patricia Martin, Susan Boyd, Matthew Best, Bradley Galgut, Peter Irwin, Paul J. Canfield, Mark B. Krockenberger, Catriona Halliday, Wieland Meyer, Richard Malik. Med. Mycology. February 2017. Quote: Pneumocystis pneumonia (PCP) is a life-threatening fungal disease that can occur in dogs. ... Te majority ofcases are currently encountered in young adult CavalierKing Charles Spaniels (CKCS). ... The aim of this study was to provide a preliminary genetic characterisation of Pneumocystis carinii f.sp.‘canis’ (P. canis) in dogs and thereby develop a reliable molecular protocol to definitively diagnose canine PCP. We investigated P. canis in a variety of lung specimens from dogs with confirmed or strongly suspected PCP (Group 1, n = 16), dogs with non-PCP lower respiratory tract problems (Group 2, n = 65) and dogs not suspected of having PCP or other lower respiratory diseases (Group 3, n = 11). Dogs with confirmed or suspected PCP (Group 1) were composed of 10 CKCS [62.5%], and one each of the following breeds or crossbreds: Kelpie, Boxer, Border collie, Chihuahua,miniature Dachshund, and Maltese/Papillion cross. ... The subcohort of CKCS ranged in age from 1 to 6 years, with a median age of 2 years and comprised six males and four fe-males. ... Presence of Pneumocystis DNA was determined by nested PCR of the large and small mitochondrial subunit rRNA loci and by a real-time quantitative polymerase chain reaction (qPCR) assay developed using a new set of primers. Molecular results were correlated with the presence of Pneumocystis morphotypes detected in cytological/histological preparations. Pneumocystis DNA was amplified from 13/16 PCP-suspected dogs (Group 1) and from 4/76 dogs of control Groups 2 and 3 (combined). The latter four dogs were thought to have been colonized by P. canis. Comparison of CT values in ‘infected’ versus ‘colonized’ dogs was consistent with this notion, with a distinct difference in molecular burden between groups (CT ≤ 26 versus CT range (26 <CT < 35), respectively). Phylogenetic analyses showed that P. canis is specifically ‘canine’ associated, being separated from other mammalian Pneumocystis species, thereby confirming the accuracy of qPCR amplicon for Pneumocystis in dogs. Using qPCR, Pneumocystis DNA can be detected in specimens from the respiratory tract and a CT value can be interpreted to distinguish infection versus colonization.
Pneumocystosis in dogs: meta-analysis of 43 published cases including clinical signs, diagnostic procedures, and treatment. Christiane Weissenbacher-Lang, Andrea Fuchs-Baumgartinger, Abigail Guija-De-Arespacochaga, Andrea Klang, Herbert Weissenböck, Frank Künzel. J. Vet. Diagn. Investig. November 2017. doi: 10.1177/1040638717742429. Quote: We evaluated 43 published cases of dogs with confirmed Pneumocystis infection [including 16 cavalier King Charles spaniels and 17 miniature Dachshunds] regarding the value of clinical parameters indicating the presence of the disease as well as tools for the detection of the pathogen. The assessed parameters included clinical signs, laboratory findings, results of thoracic radiography, autopsy, histopathology, methods for the detection of Pneumocystis, as well as medical therapy. Pneumocystosis was diagnosed most often in certain breeds (Cavalier King Charles Spaniel, Miniature Dachshund) with a predisposition for impaired immunity. ... A breed predisposition for Miniature Dachshunds and Cavalier King Charles Spaniels is evident. Dachshunds are reported to have a predisposition for combined B- and T-cell immunodeficiency, and typical clinical after-effects, such as severe respiratory tract infections, are documented. Given that Cavalier King Charles Spaniels were more susceptible to pneumocystosis than other breeds, a similar impairment of immunity was also assumed, but has not yet been confirmed. In a 2009 study, 2 King Charles Cavalier Spaniel littermates were affected by pneumocystosis, which also supports suspicions of an underlying heritable immunodeficiency in this breed. ... The median age of the dogs was 1 y. Chronic therapy-resistant respiratory signs, such as tachypnea, dyspnea, and cough, along with leukocytosis, neutrophilia, and hypogammaglobulinemia, were the most frequently described clinical and clinicopathologic abnormalities. Pneumocystosis can be masked by coinfections with other respiratory pathogens, and the successful detection of Pneumocystis organisms is of major relevance. Several detection methods have been used in the past, but only a few provide reliable results. In 2017, the cytologic evaluation of Giemsa-stained bronchoalveolar lavage samples is generally used, even if sensitivity is only moderate. More reliable results can be achieved using special stains or sensitive molecular techniques. Fast and reliable detection of Pneumocystis is the essential basis for appropriate treatment and higher survival chances for dogs. ... The administration of an immunosuppressive dose of prednisolone of 15 mg q12h has only been described once in a Cavalier King Charles Spaniel. Because pneumocystosis occurs only rarely in dogs, there is little experience with the regulation of corticosteroid concentrations and the balance between immunosuppression and proliferation of the fungus. Additionally, predisposition for Pneumocystis infections of dog breeds with inherited immunodeficiency should be considered in the choice of an appropriate therapy.
Diagnosis of pneumocystis pneumonia in a 2-year-old King Charles Cavalier Spaniel using the polymerase chain reaction. Ayeley A. K. Okine, Seth Chapman, Roger A. Hostutler, Robert Livingston. Vet. Clin. Pathol. March 2018;47(1):146-149. Quote: A 2-year-old, female spayed, King Charles Cavalier Spaniel was presented for evaluation of dyspnea, inappetence, and lethargy. Thoracic radiographs revealed a moderate diffuse interstitial lung pattern affecting the perihilar and caudodorsal lung fields, and an echocardiogram revealed severe pulmonary hypertension. A bronchoalveolar lavage (BAL) was performed, and cytology revealed mixed inflammation with cysts and trophozoites consistent with Pneumocystis. Pneumocystis infection was later confirmed with PCR. To the author's knowledge, this report represents the first case of canine pneumocystis pneumonia diagnosed antemortem with PCR from a BAL sample. Pneumocystis represents an important, but uncommon cause of afebrile pneumonia in immunosuppressed dogs.
The diagnostic approach to coughing in dogs and cats. Jenny Reeve. Companion Anim. July 2018;23(7):396-404. Quote: Coughing is a common presenting sign in dogs, less so in cats, and may be a manifestation of a wide range of disorders, from acute self-limiting disease that does not require specific diagnosis and treatment, through to acute and chronic diseases of varying severity that require appropriate investigation to guide optimal management and outcome. This article reviews the diagnostic approach to coughing. ... Table 1. Causes of coughing with associated commonly affected breeds: ... Pneumocystis carinii infection: Cavalier King Charles Spaniel, Dachshund.
CT findings in Pneumocystis carinii pneumonia in five dogs. F. Schiborra, C. J. Scudder, R. M. Littler, C. R. Lamb, J. F. McConnell, T. W. Maddox. J. Sm. Anim. Pract. August 2018;59(8):508-513(6). Quote: Pneumocystis carinii pneumonia is a rare disease in dogs. It is primarily reported in cavalier King Charles spaniels and miniature dachshunds with suspected underlying immunodeficiency. This case series reports the findings in five dogs (four cavalier King Charles spaniels and one Bedlington terrier) with confirmed P. carinii pneumonia. Thoracic (CT) revealed ground glass opacity of the pulmonary parenchyma with a diffuse or multifocal distribution. The severity of this pattern was variable. Less consistent imaging findings included parenchymal bands, bronchial dilation and signs consistent with pulmonary hypertension. Four dogs recovered well with treatment and there was resolution of CT abnormalities in all dogs with follow-up.
Confirmed case of Pneumocystis pneumonia in a Maltese Terrier × Papillon dog being treated with toceranib phosphate. MP Best, SP Boyd, Danesi. Australian Vet. J. May 2019;97(5):162-165. Quote: A 7-year-old female-neutered Maltese Terrier × Papillon dog was presented with tachypnoea and weight loss following 12 months of therapy with toceranib phosphate for a metastatic, histologically-low-grade mast cell tumour. The dog was diagnosed with Pneumocystis canis based on PCR with supportive clinical, radiographic and cytological findings. No other clinical evidence of immunocompromise was identified through assessment of haematology and immunoglobulin quantification. Clinical signs completely resolved with a short course of potentiated sulfonamides and discontinuation of the toceranib. Conclusion: To the authors’ knowledge this represents the first case of Pneumocystis in a dog secondary to immunomodulatory drug therapy. It is also the first case of opportunist infection secondary to a tyrosine kinase inhibitor in dogs. ... Dachshunds and Cavalier King Charles Spaniels are by far the most commonly reported breeds. Most cases present at less than 2 years of age, although Cavalier King Charles Spaniels can present at a slightly older age with one case recorded in a 6-year old dog.
Nested–polymerase chain reaction detection of Pneumocystis carinii f. sp. canis in a suspected immunocompromised Cavalier King Charles spaniel with multiple infections. Matteo Petini, Tommaso Furlanello, Patrizia Danesi, Andrea Zoia. SAGE Open Med. Case Rpts. April 2019;7:1-5. Quote: A 7-month-old Cavalier King Charles Spaniel female was referred due to a chronic cough refractory to antibiotic treatments. Laboratory findings showed leukocytosis, increased serum C-reactive protein, hypogammaglobulinemia, and decreased total serum immunoglobulin G concentration. Thoracic radiographs showed a mild bronchial pattern. Cytology of the bronchoalveolar lavage fluid revealed a septic inflammation. Bordetella bronchiseptica, Mycoplasma spp., and Pneumocystis carinii were identified by polymerase chain reaction testing, and Klebsiella pneumonia was cultured from the bronchoalveolar lavage fluid. Moreover, Escherichia coli was also cultured from urine. Pneumocystis spp. identification was done by sequencing of genetic amplicons. The dog died due to cardiopulmonary arrest secondary to a spontaneous pneumothorax on the day following the procedure. This report documents the detection of Pneumocystis carinii f. sp. canis in a suspected immunocompromised Cavalier King Charles Spaniel with concurrent pulmonary and urinary tract infections involving four different pathogens, and highlights the importance of the use of polymerase chain reaction testing to detect canine Pneumocystis spp. in cases with negative bronchoalveolar lavage cytology. ... While signalment, medical history, clinicopathological, and nested PCR findings supported a PP diagnosis in our dog, the radiographic findings were not consistent with PP. However, in human medicine, it is strongly recommended to consider the detection of Pneumocystis spp. DNA in symptomatic patients, whatever the fungal load, to be at least partially, responsible for the clinical signs.
Genomic insights into the host specific adaptation of the Pneumocystis genus. Ousmane H. Cissé, Liang Ma, John P. Dekker, Pavel P. Khil, Jung-Ho Youn, Jason M. Brenchley, Robert Blair, Bapi Pahar, Magali Chabé, Koen K. A. Van Rompay, Rebekah Keesler, Antti Sukura, Vanessa Hirsch, Geetha Kutty, Yueqin Liu, Li Peng, Jie Chen, Jun Song, Christiane Weissenbacher-Lang, Jie Xu, Nathan S. Upham, Jason E. Stajich, Christina A. Cuomo, Melanie T. Cushion, Joseph A. Kovacs. Commun. Biol. March 2021; doi: 10.1038/s42003-021-01799-7. Quote: Pneumocystis jirovecii, the fungal agent of human Pneumocystis pneumonia, is closely related to macaque Pneumocystis. Little is known about other Pneumocystis species in distantly related mammals, none of which are capable of establishing infection in humans. The molecular basis of host specificity in Pneumocystis remains unknown as experiments are limited due to an inability to culture any species in vitro. To explore Pneumocystis evolutionary adaptations, we have sequenced the genomes of species infecting macaques, rabbits, dogs and rats and compared them to available genomes of species infecting humans, mice and rats. ... P. canis samples were obtained as DNA from one Cavalier King Charles Spaniel dog at the University of Helsinki, Finland and one Whippet mixed-breed at the University of Veterinary Medicine, Vienna, Austria. The dogs were not laboratory animals. ... Complete whole genome sequence data enables analysis and robust phylogeny, identification of important genetic features of the host adaptation, and estimation of speciation timing relative to the rise of their mammalian hosts. Our data reveals insights into the evolution of P. jirovecii, the sole member of the genus able to infect humans.
Pneumocystis Colonization in Dogs Is as in Humans. Patrizia Danesi, Matteo Petini, Christian Falcaro, Michela Bertola, Elisa Mazzotta, Tommaso Furlanello, Mark Krockenberger, Richard Malik. Int. J. Environ. res. Public Health. March 2022; doi: 10.3390/ijerph19063192. Quote: Pneumocystis is an atypical fungus that resides in the pulmonary parenchyma of many mammals, including humans and dogs. Immunocompetent human hosts are usually asymptomatically colonised or show subtle clinical signs, but some immunocompromised people can develop florid life-threatening Pneumocystis pneumonia (PCP). Since much less is known concerning Pneumocystis in dogs, we posit the question: can Pneumocystis colonization be present in dogs with inflammatory airway or lung disease caused by other pathogens or disease processes? ... It is important to state that the overall prevalence of symptomatic PCP in canine populations is very low, except in two pedigree populations viz. CKCS and miniature Dachshunds. ... The cohort of dogs included in this study was composed of 70 crossbred dogs and 185 pedigree (purebred) dogs, with ages ranging from very young (<one-year-old) to 16 years and with males over-represented (Figure 1). Among the 64 different breeds and hybrids, Labrador retrievers and Cavalier King Charles Spaniels (CKCS) were most common, comprising 14 and 10 dogs, respectively; other breed(s) numbered less than 10 dogs each. ... In this study, Pneumocystis DNA was detected in bronchoalveolar lavage fluid (BALF) of 22/255 dogs (9%) with respiratory distress and/or chronic cough. ... The positive pedigree breeds consisted of: Boxer dogs (n = 3; 14%), CKCS (n = 2; 9%), Pomeranian (n = 2; 9%) and one each of various other breeds (Figure 1). In this cohort, 16/22 (73%) of dogs were young (≤1 year old), while the remaining six dogs were 5 to 11 years old. There were 17 male dogs and five females. To summarise the P. canis qPCR-positive cases, but placed into conceptual categories, there was: CKCS with Bordetella bronchiseptica, Mycoplasma spp. and low Ct for P. canis, but no data on response to therapy (1), CKCS with P. canis with Bordetella bronchiseptica but no data on response to therapy (1) ... Although young dogs (<1 year-of-age) and pedigree breeds were more often Pneumocystis-qPCR positive than older dogs and crossbreds, adult dogs with other infectious conditions and/or a history of therapy-resistant pulmonary disease could also be qPCR-positive, including two patients with suppression of the immune system. ... Generally, there are two canine breeds well known to be at increased risk for the development of PCP, viz. the CKCS and the Miniature Dachshund. ... Absence of pathognomonic clinical or radiographic signs render it impossible to convincingly discriminate between overt PCP versus other lung/airway disease processes colonised by P. canis. It is possible that colonisation with P. canis might play a certain role as a co-pathogen in some canine patients with lower respiratory disease.
Pneumocystis spp Pneumonia in a Dog. Brandon Verkinderen, Lisa M. Pohlman. Clinician's Brief. December 2023. Quote: A 20.1-lb (9.1-kg), 2-year-old intact male Cavalier King Charles spaniel was presented for progressively increased respiratory effort of ≈2- to 3-weeks’ duration. The patient had been seen at a different clinic 2 weeks prior when the owner first noted tachypnea. Thoracic radiographs at that time revealed a diffuse interstitial to alveolar pattern. ... Pneumocystis spp are opportunistic fungi, previously classified as protozoa, that have an evolutionary history of adaptation to commensal status within the pulmonary parenchyma. ... Heart rate was 96 bpm; a heart murmur was not present. Respiration rate was 120 breaths per minute, and increased inspiratory effort was observed. ... Thoracic radiographs revealed a diffuse mixed bronchial and interstitial pattern most consistent with an infectious cause. ... Upper airways appeared normal on bronchoscopy, and the BAL sample was submitted to clinical pathology for evaluation. Cytocentrifuged slide preparations of BAL fluid revealed neutrophils; variably vacuolated macrophages; numerous extracellular, small, pale blue, crescent- to ovoid-shaped trophozoites with small blue nuclei; and scattered extracellular, round, pale cysts that contained multiple trophozoites. Occasional intracellular organisms were also identified within macrophages. ... Treatment & Management: Sulfadiazine/trimethoprim (30 mg/kg PO every 12 hours for 21 days), dexamethasone (0.15 mg/kg IV every 24 hours for 3 days), and theophylline (11 mg/kg PO every 12 hours for 14 days) were administered. Trazodone (3 mg/kg PO every 8-12 hours as needed for 14 days) was administered for sedation during the treatment period. The patient was discharged after 4 days in the hospital, and a 3-week recheck examination with thoracic radiography was recommended. ... Pneumocystis spp can subclinically colonize lung tissue but proliferate uncontrollably in immunocompromised patients, resulting in severe, clinical, life-threatening pulmonary disease (ie, Pneumocystis spp pneumonia, pneumocystosis). Transmission and development of pneumocystosis results from environmental exposure or contact between airborne droplets from colonized subjects and susceptible immunosuppressed patients within a species.1,4 Pneumocystis spp organisms settle and proliferate in the lower respiratory tract, leading to inflammation, alveolar–capillary blockage, decreased gaseous exchange, and pulmonary alveolar damage. Clinical Presentation: Pneumocystis spp pneumonia is reported in various dog breeds but overrepresented in young miniature dachshunds and Cavalier King Charles spaniels, with a majority of clinical infections due to underlying immunodeficiency (eg, immunoglobulin deficiencies).2,3 Patients are typically presented with afebrile pneumonia and variable clinical signs, including tachypnea, dyspnea, cough, cyanosis, inappetence, and exercise intolerance. Diagnostics: Hematologic abnormalities are often nonspecific, usually consisting of a leukocytosis characterized by neutrophilia, monocytosis, and eosinophilia (uncommon).4,5 Serum chemistry profile changes are also typically nonspecific, except for hypoglobulinemia or hypogammaglobulinemia.4 Immunoglobulin (Ig) findings typically include decreased to normal IgG concentration (often lower than in healthy dogs) and increased or normal IgM concentration (often higher than in healthy dogs).2,5 This shift in Ig concentration is attributed to a selective defect in IgG that results in dogs infected with P canis having a more proliferative IgM response compared with IgG.2,5 Determining Ig concentrations via serum electrophoresis may be beneficial in patients with suspected Pneumocystis spp infection. Thoracic radiography is also relatively nonspecific for Pneumocystis spp pneumonia; findings include a diffuse, bilaterally symmetric, interstitial to alveolar lung pattern. Although findings are nonspecific, thoracic radiography is recommended to evaluate extent of disease and assess for pneumomediastinum or pneumothorax, which are common complications of pneumocystosis. BAL and cytology using a Romanowsky-type (eg, 3-step, Wright’s, modified Wright’s, Giemsa) stain, new methylene blue, or Gram stain can allow for identification and definitive diagnosis of pneumocystosis. Cyst or trophozoite forms of the organism may be identified on cytology. Cysts range from 5 to 10 μm in diameter and typically contain 4 to 8 basophilic bodies, often arranged in a circle. Trophozoites are pleomorphic, with a length of 2 to 7 μm. If the organism is not identified with BAL and cytology, additional diagnostics (eg, PCR) have a high sensitivity for detection of Pneumocystis spp organisms and can be performed using the BAL fluid sample.1 If the BAL sample is nondiagnostic, an invasive procedure to acquire a lung biopsy can be performed. Treatment & Prognosis: Pneumocystis spp pneumonia has a guarded prognosis, and treatment success depends on early diagnosis and immediate initiation of aggressive therapy.1 Any underlying illness should also be treated. Pneumocystis spp are classified as fungi but are resistant to most antifungal drugs and susceptible to antiprotozoal drugs. The most common therapeutic regimen includes a combination of antimicrobials and corticosteroids. The antimicrobial of choice is sulfa-/trimethoprim (30 mg/kg PO every 12 hours for 3 weeks or 15 mg/kg PO every 8 hours for 3 weeks [less common]). Corticosteroids are indicated because respiratory disease and mortality are more associated with extent of inflammation than burden of organisms. Corticosteroids must be administered at low, anti-inflammatory dosages that improve pulmonary function and increase the chance of survival but do not facilitate replication of the fungus. Prednisone (anti-inflammatory dose, 0.3-0.5 mg/kg PO every 12 hours for ≤3 days) is the oral corticosteroid of choice. Tapering is not necessary because of the relatively low dose and short duration of use (<1 week). Supportive care (eg, bronchodilators, oxygen therapy) is also typically provided for initial treatment and stabilization.
A Novel CARMIL2 Immunodeficiency Identified in a Subset of Cavalier King Charles Spaniels with Pneumocystis and Bordetella Pneumonia. Emily L. Coffey, Liang Ma, Ousmane H. Cissé, Joseph A. Kovacs, Katie M. Minor, Antti Sukura, Patrizia Danesi, Steven G. Friedenberg, Jonah N. Cullen, Christiane Weissenbacher-Lang, Julie C. Nadeau, Amber M. Graham, Martin N. Granick, Natalie K. Branson, Kyle C. Branson, Barbara Blasi, Casandra M. Jacobs, Eva Furrow. J. Fungi. March 2024; doi: 10.3390/jof10030198. Quote: Pet dogs are a valuable natural animal model for studying relationships between primary immunodeficiencies and susceptibility to Pneumocystis and other opportunistic respiratory pathogens. Certain breeds, such as the Cavalier King Charles Spaniel, are over-represented for Pneumocystis pneumonia (PCP), suggesting the presence of a primary immunodeficiency in the breed. Here, we report the discovery of a CARMIL2 nonsense variant in three Cavalier King Charles Spaniel dogs with either PCP (n = 2) or refractory Bordetella pneumonia (n = 1). CARMIL2 encodes a protein that plays critical roles in T-cell activation and other aspects of immune function. Deleterious CARMIL2 variants have recently been reported in human patients with PCP and other recurrent pneumonias. In addition to opportunistic respiratory infection, the affected dogs also exhibited other clinical manifestations of CARMIL2 deficiencies that have been reported in humans, including early-onset gastrointestinal disease, allergic skin disease, mucocutaneous lesions, abscesses, autoimmune disorders, and gastrointestinal parasitism. ... Prior to this study, whole genome sequencing (Illumina HiSeq2500 platform with 150-base paired-end reads) was performed on a respiratory sample obtained from a CKCS previously diagnosed with PCP (dog 1; D1). ... After identification of the CARMIL2 variant in D1, genotyping was performed to screen additional dogs from three phenotypic cohorts. The first cohort consisted of 11 CKCSs with a suspected PI based on a diagnosis of PCP or recurrent pneumonia from other respiratory pathogens. DNA from nine of these dogs was submitted to the University of Minnesota Canine Genetics Laboratory (UMN CGL) for genetic testing for a PI, while DNA from the other two dogs came from a collection at the National Institutes of Health (NIH) from previous research on PCP in dogs [13]. The second cohort included 15 dogs of other (not CKCSs) or unknown breeds that were previously diagnosed with PCP. ... The final cohort included 115 control CKCSs with no PCP or clinical suspicion of a PI. ... The canine CARMIL2 protein consists of 1394 amino acids; the p.R291* variant identified here results in a loss of 79% of the protein sequence. ... Of the 21 CKCS dogs in the internal database of whole genome sequencing variant calls, 1 was heterozygous, and 20 were clear of the CARMIL2 variant. Of the 115 control CKCS dogs genotyped by the UMN CGL, 12 were heterozygous and 103 were clear of the variant. The variant allele frequency in the combined group of CKCS database and control dogs was 4.8% (95% CI 2.8–8.0%). The 559 dogs of other breeds in the internal database were all homozygous for the reference allele. ... Dog 2 (D2) was a neutered male CKCS diagnosed with PCP at 16 months of age via PCR testing of a deep oropharyngeal swab. Immunoglobulin assays showed all values within the normal reference intervals (IgM: 350 mg/dL, RI: 100–400 mg/dL; IgG: 1200 mg/dL, RI: 670–1650 mg/dL; IgA: 240 mg/dL, RI: 35–270 mg/dL). Treatment with a 6-week course of TMS (30 mg/kg every 8 h) and an anti-inflammatory dose of prednisone (0.5 mg/kg/day) resulted in resolution of both clinical and radiographic manifestations. After completing TMS therapy, no prophylaxis to prevent recurrence was given. At the time of writing, one year after PCP diagnosis, the patient has not had any relapses of respiratory infection. Additional medical history included chronic diarrhea, atopic dermatitis, an anal gland abscess, and gastrointestinal (GI) parasitism. Dog 3 (D3) was an intact male CKCS that suffered from a chronic cough since approximately 2 months of age. He was diagnosed with pneumonia secondary to Bordetella bronchiseptica and Mycoplasma cynos infections at 5 months of age. The diagnosis was made by a PCR panel, cytology, and cultures of endotracheal wash fluid. Pneumocystis PCR of the fluid was negative. Prednisone (1 mg/kg/day) and doxycycline therapy (5 mg/kg every 12 h) provided an initial clinical improvement in cough and respiratory effort, though the effects were transient. Bronchoscopy and BAL were performed, and the patient was diagnosed with persistent Bordetella infection via culture of the lavage fluid. The patient was then given gentamicin nebulization and enrofloxacin (10 mg/kg/day). At the time of writing, four months after initiating therapy, the patient was still receiving inhaled gentamicin. His respiratory signs have improved overall, though he still experiences an intermittent cough and exercise intolerance. Additional medical history included chronic hypocholesterolemia with mixed bowel diarrhea, giardiasis, coccidiosis, coprophagia, and masticatory muscle myositis (MMM), which was diagnosed at 3 months of age. No other causes of acquired immunodeficiency (e.g., immunosuppressive medication) were noted for any of the three dogs. ... Nine CKCSs with suspected PI (six males and three females) tested clear of the CARMIL2 p.R291* variant. The median age was four months (range: three months–six years), with all dogs less than one year old except for one. All dogs had a history of respiratory signs that were characterized as chronic, recurrent, or refractory to therapy. Respiratory pathogens identified included Pneumocystis alone in two dogs, Bordetella alone in one dog, and co-infections of Pneumocystis and Bordetella in one dog, Bordetella and Mycoplasma in three dogs, and Bordetella and Pasteurella in one dog. No other causes of acquired immunodeficiency were identified for any dogs. ... This study reports the presence of a combined immunodeficiency caused by a CARMIL2 variant in three CKCSs with PCP or refractory Bordetella pneumonia. These CKCSs also suffered from non-respiratory clinical manifestations that parallel CARMIL2 immunodeficiencies in humans. Given the rarity of CARMIL2 immunodeficiencies in humans, data from naturally affected dogs might expand the understanding of biological and clinical outcomes for this condition in both species. Furthermore, genetic testing of CKCSs for the CARMIL2 variant can aid in clinical diagnosis of a PI and guide breeding practices, thus reducing the frequency of this specific immunodeficiency in the breed. Collectively, these results demonstrate the value of a natural canine model for studying the interplay between PIs, host immune responses, and Pneumocystis susceptibility.
Pneumocystis pneumonia diagnosed by PCR performed from an oropharyngeal swab in a Cavalier King Charles Spaniel: Case report. Julie Nadeau, Amber Graham, Robyn Sherman. Vet. Rec. Case Rpts. March 2025; doi: 10.1002/vrc2.70020. Quote: A 16-month-old Cavalier King Charles Spaniel presented to a private referral practice with a history of progressive tachypnoea, acute syncopal episode, increased respiratory effort and weight loss that failed to respond to empirical antimicrobial management and traditional antifungal therapy. The dog was diagnosed with Pneumocystis pneumonia by polymerase chain reaction performed from an oropharyngeal swab and secondary pulmonary hypertension was diagnosed with echocardiography. Clinical signs resolved with trimethoprim-sulfonamide, an anti-inflammatory prednisone tapering course, and sildenafil with tapering course for pulmonary hypertension. This is the first case report documenting Pneumocystis pneumonia diagnosed via oropharyngeal swab, with complete resolution of clinical signs and eventual cessation of all medications.
CONNECT WITH US